Contraception
In this day and age, there are many different ways of contraception and patients should be told about all of their options so the best fit can be found. In general, more invasive contraceptives are also the most effective and the effectiveness of contraception is usually defined/measured at a population level, rather than the individual level (E.g. barrier contraception is very effective if an individual commits to using it properly, but most of the population does not use it properly or each time).
- Highly effective
- Long-acting reversible contraception (LARC)
- Most effective for a patient who desires to not get pregnant
- Types
- Non-IUD
- Effective for 3 years
- Placed under the skin
- Nexplanon
- Implanon
- Implantable uterine device (IUD)
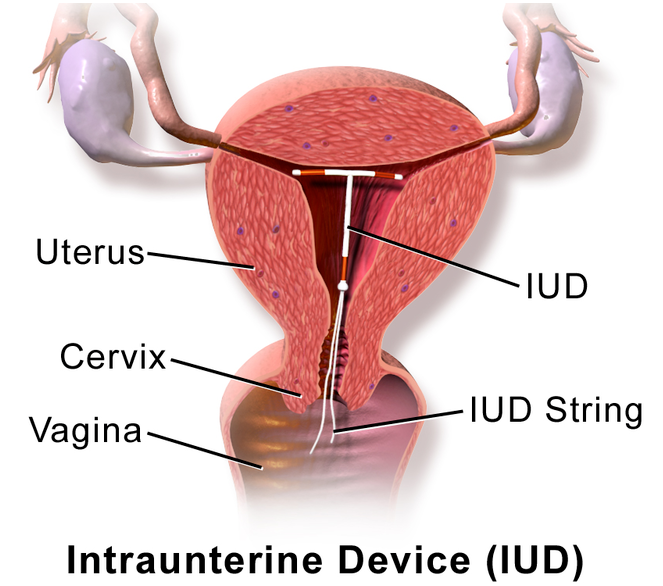
- Hormonal
- Last for 5 years
- Estrogen and progesterone = increased DVT risk
- Bleeding decreased or stopped
- Copper

- Longest acting = 10 years
- No hormones
- May result in increased bleeding
- Non-IUD
- Non-reversible contraception
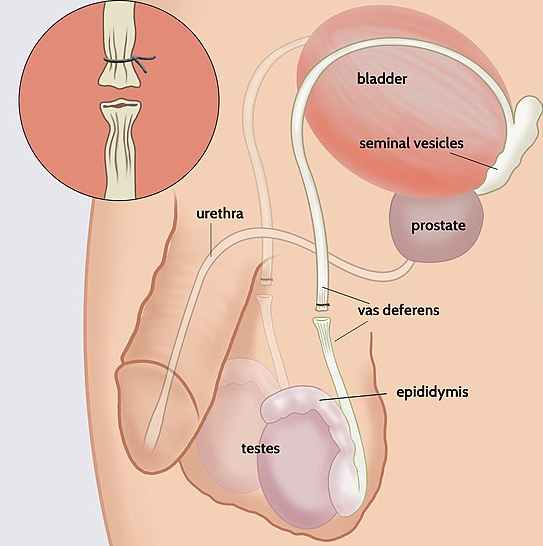
- Vasectomy
- Bilateral tubal ligation
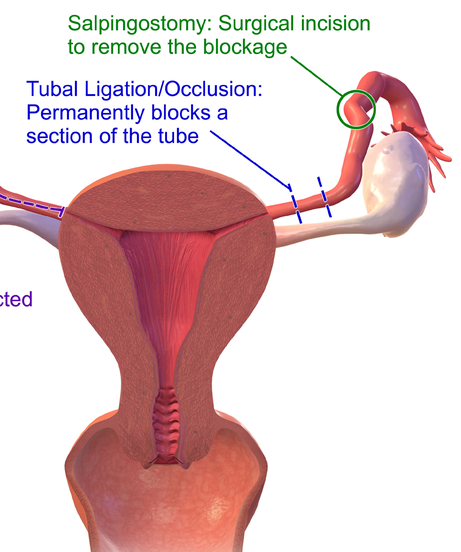
- Can be completed during a C-section
- Not 100% effective
- Possibility of an ectopic pregnancy
- Vasectomy
- Long-acting reversible contraception (LARC)
- Moderately effective
- Injections
- "Provera"

- Can last 3 months
- Best for women who want to be non-fertile for a temporary amount of time but may not be compliant on the daily
- Patches
- "Ortho-Eura"
- Can last 1 month
- Can fall off
- The highest risk of DVT/PE
- Any contraception containing estrogen will increase this risk
- Age >35 is a higher risk for VTE
- Actively smoking is a higher risk for VTE
- Rings
- Estrogen and progesterone
- Can last 1 month
- Placed into the vagina
- Can fall out or cause discomfort during intercourse
- OCPs

- Estrogen and progesterone
- Not the best choice for contraception
- Require daily compliance
- If contraception is desired LARC is better
- Very useful in disorders
- Uterine bleeding
- Gestational trophoblastic disease
- Progesterone only
- DVT risk not as high
- Also requires daily compliance
- Even tighter compliance than the OCP
- Injections
- Low effective - very effective for single-use, not over the long term
- Barrier methods
- The advantage of these is sexually transmitted disease protection
- Types
- Condoms - males
- Quick

- Diaphragm - females
- Needs to be placed in advance = slow
- Condoms - males
- Non-barrier
- No STI protection
- Not as effective for contraception
- Use these in addition to barrier contraception if you choose to
- Types
- Spermicide
- ???????

- ???????
- Sponge
- Caps
- Spermicide
- Barrier methods
- Not very effective
- Family planning
- Doesn't work for avoiding pregnancy
- Used for getting pregnant
- Withdrawal
- Male controlled
- Pre-ejaculate can result in pregnancy still
- Abstinence
- Highly effective if done, but on a population level not effective
- Family planning
- Post intercourse
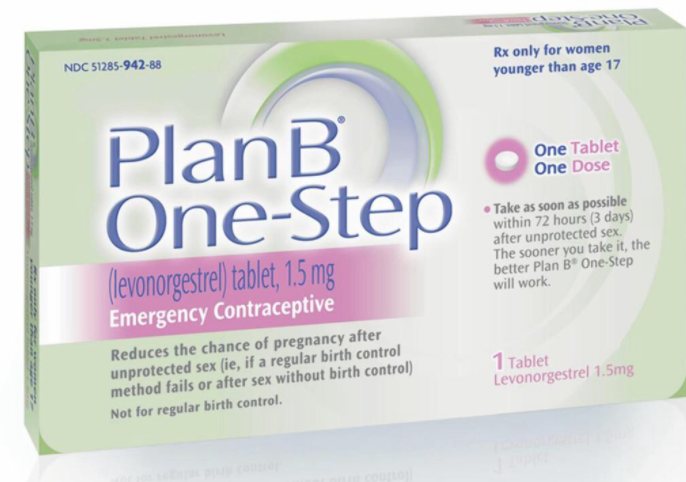
- Levonorgestrel - "Plan B"
- Must be used within 72 hours of intercourse
- Will prevent pregnancy but not result in an abortion if one has started
All information provided on this website is for educational purposes and does not constitute any medical advice. Please speak to you doctor before changing your diet, activity or medications.
