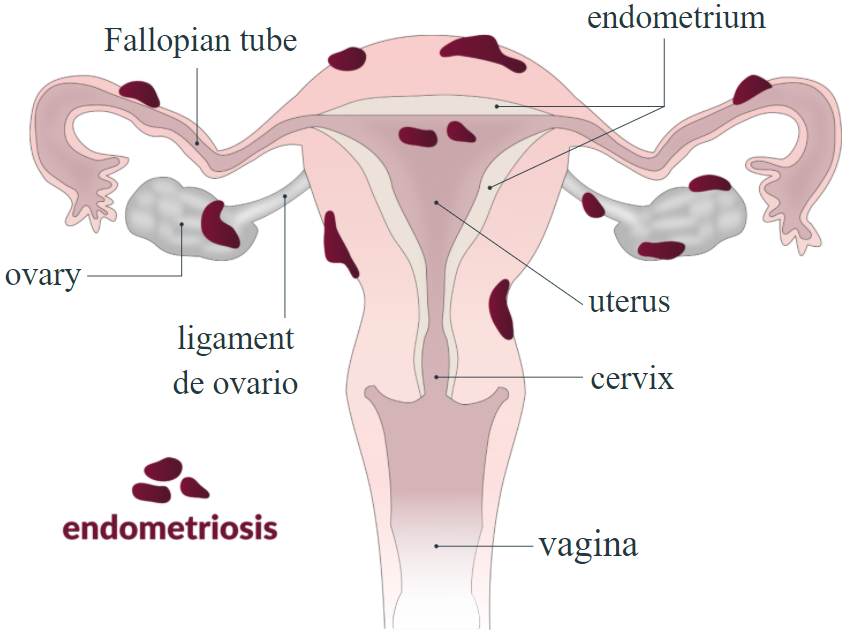
Endometriosis
Endometriosis is the presence of endometrial tissue outside the uterus and affects 5-10% of women of reproductive age and up to 40% of infertile women. Chronic pelvic pain is a prevalent symptom. There are multiple possible mechanisms for the development of endometriosis
- Retrograde menstruation
- Endometrial tissue moves back up the fallopian tubes during menstruation instead of anterograde into the vagina
- Celomic metaplasia
- Cells outside the uterus undergo a change and turn into endometrial cells
- Hematogenous dissemination
- Endometrial cells spread to outside of the uterus through the blood (similar to cancer cells)
- Autoimmune disease
- Problem in the immune systems allows the endometiral cells to roam free and seek new places to grow in
Symptoms
Although many of the patients with endometriosis are asymptomatic, cyclical pelvic pain and infertility are 2 of the most common symptoms. Additonally many women experience the 4 "D"s of endometriosis:
- Dysmenorrhagia
- Onset with menstruation or just before
- Dysperonea
- Pain wit intercourse
- Dyskinesia
- Pain with defecation
- Dysurea
- Pain with urination
- Infertility (sorry not a "D", but still important)
In general the degree of pain is not an indication of the degree of pelvic disease. The cause of infertility is not known well, but sometimes can be due to the pelvic anatomic distortion due to extensive endometriosis.
Diagnosis
The most common site of endometriosis is the ovaries and as such physical exam (adnexal tenderness) and history (cyclical pain) can often direct towards the correct diagnosis of endometriosis.
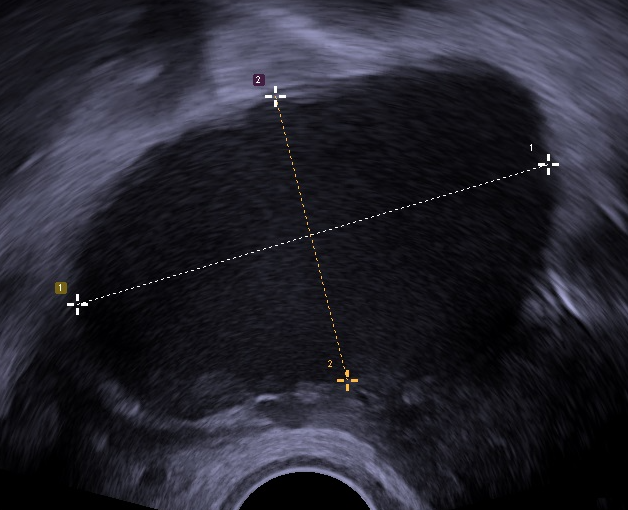
- Ultrasound
- Endometriomas (blood filled ovarian cysts) can sometimes be visualized
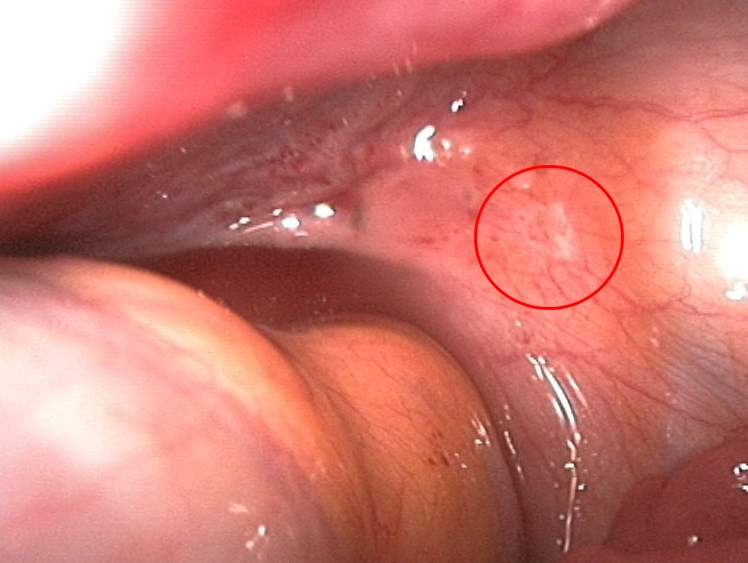
- Laparoscopic surgery
- The gold standard with direct visualization of the extrauterine endometrial tissue
- Biopsies can be taken for confirmation
- Endometrial lesions can be small and vesicular (early) or have a powder-burn appearance (late)
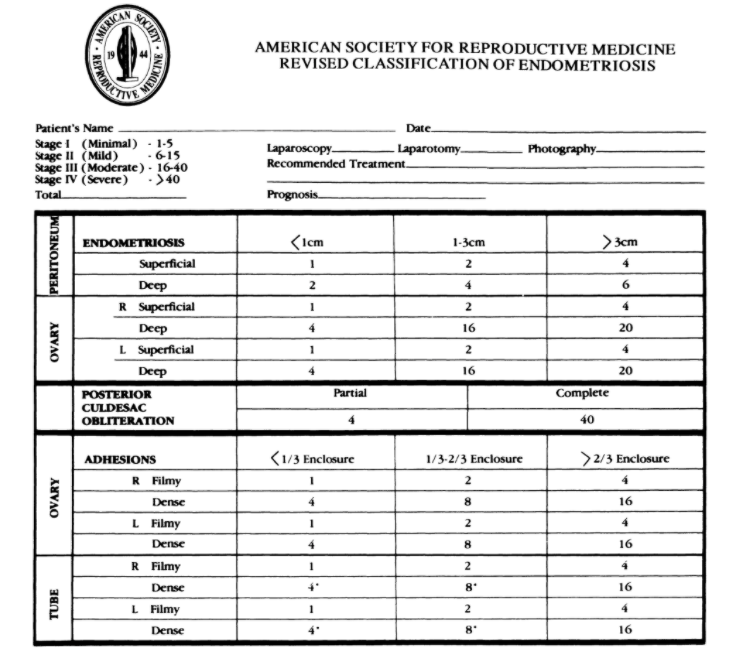
Classification
The American fertility society scoring system taken into account a number of surgical findings to estimate the severity of disease.
Management
- Medical management
- Meant to induce amenorrhea and provide symptomatic relief
- Patients initially receive a trial of NSAIDS and OCPs as a trial. If this fails to work, diagnostic surgery is warranted (discussed below)
- NSAIDS
- Pain control and reduce menstrual flow (through prostoglandin inhibition)
- Opiates
- For more severe pain control
- Progestin
- Do the opposite of what estrogen does
- "Thins" out the endometrial tissue and inhibits growth
- Can induce amenorrhea
- Oral contraceptive pill (OCP)
- Used to eliminate or reduce menstrual flow
- Danazol
- Strong steroid used to inhibit endometrial tissue growth
- Can cause hirsutism as a side effect
- GnRH agonists
- Hypoestrogenic menopause
- Symptoms of menopause can be unpleasant
- Can lead to osteoporosis
- Estrogen therapy can be added on the side to counteract the adverse side effects
- Surgical management
- This is used for diagnosis if management with NSAIDs and OCPs fails
- Laparoscopic surgery is also used for therapeutic purposes while maintaining fertilityin young women
- Goal is total excision of the endometrial tissue outside the uterus
- Endometrioma >4cm or pelvic adhesions are indications for laparoscopic management
- Older women who are not concerned about pregnancy can undergo hysterectomy and bilateral salpingioopheroctomy (more definitive treatment)
- Pain can sometimes persist post surgery and medical management is still warranted
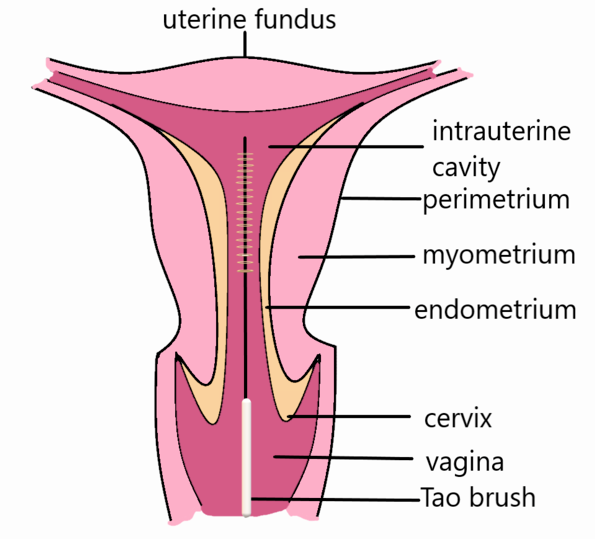
Adenomyosis
This condition is very similar to endometriosis but involves the presence of endometrial tissue within the myometrium (still in the uterus). Prevelance of this condition is even higher than endometriosis at 20%.
Symptoms can include chronic pelvic pain with menorrhaia and dyspareunia.
Diagnosis
Definitively done via biopsy. Ultrasound maybe suggestive of diagnosis however.
Treatment
- Medical
- OCPs
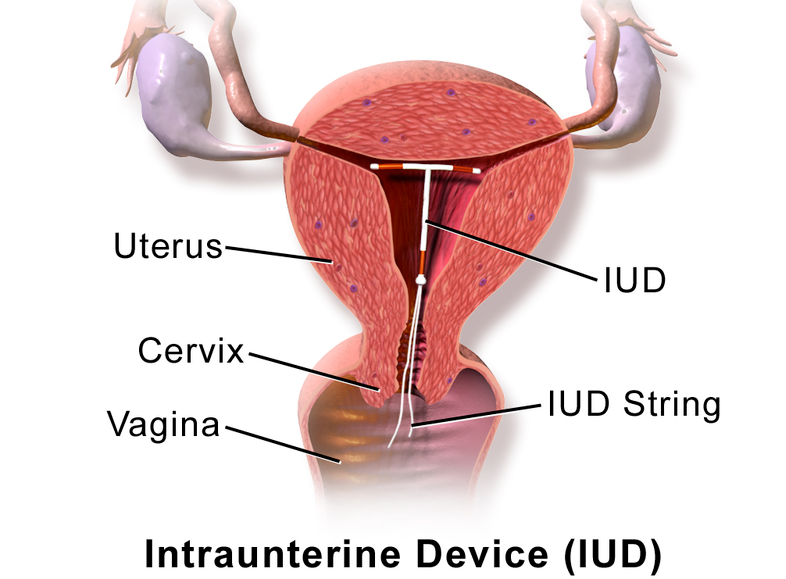
- Mirena (IUD)
- Surgical management
- Hysterectomy
All information provided on this website is for educational purposes and does not constitute any medical advice. Please speak to you doctor before changing your diet, activity or medications.
