Miscarriage
Miscarriage is the expulsion of the fetus from the uterus before it is capable of sustaining life independently. Interestingly, 50-75% of all conceptions end in a miscarriage but most go unnoticed because they occur before or during the subsequent period.
Spontaneous miscarriage
Loss of pregnancy before 20 weeks gestation or <500g mass. Advanced maternal age, prior miscarriages and smoking are the most significant risk factors. Most pregnant women experience vaginal bleeding followed by lower abdominal cramping. A physical exam should include vital sign assessment (for hemodynamic instability), a speculum exam (to assess the cervix) and a bimanual exam to estimate the gestational age.
Management should include Rh blood typing and all Rh-negative patients should receive anti-D immunoglobulin prophylaxis.
Etiology
Most of the pregnancies ending with a miscarriage do so within the first trimester. The fetus is often already dead by the time of expulsion. At least half of these fetuses die due to chromosomal abnormalities. Second trimester miscarriages are more likely to result from anatomic factors and the fetus is usually not dead by the time of expulsion.
- Fetal factors
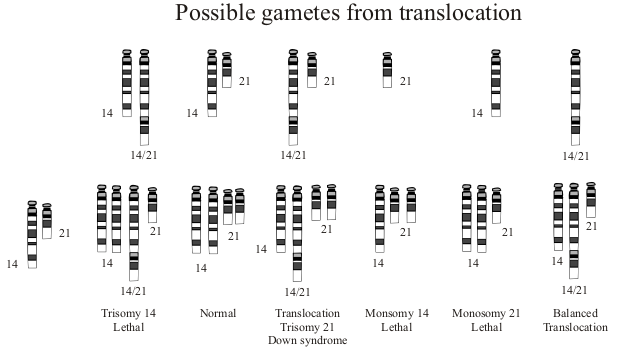
- Chromosomal issues
- Autosomal trisomies are the most common cause (13, 16, 18, 21, 22)
- Monosomy X is the second most common cause
- Developmental issues
- Common in first trimester miscarriages
- Chromosomal issues
- Maternal factors
- Uterine defects
- Fibroids are usually not the cause of miscarriages
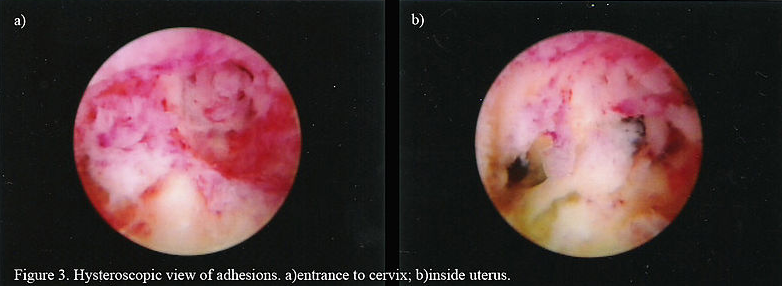
- Asherman syndrome (from multiple curettages) can make the endometrium insufficient to host a pregnancy
- Incompetent cervix is a correctable cause of miscarriages
- Infections
- Endocrine issues
- Immune reasons
- Trauma
- Especially abdominal trauma
- Uterine defects
Classification
| Miscarriage | Symptoms | Pelvic exam | Ultrasound findings |
|---|---|---|---|
| Threatened |
Mild vaginal bleeding Mild abdominal pain Membranes intact Fetal cardiac activity important |
Cervix closed | Intrauterine pregnancy viable |
| Inevitable |
Vaginal bleeding and abdominal pain Membranes may be broken or non-broken |
Cervix open | Pregnancy mostly non-viable |
| Incomplete |
Heavy vaginal bleeding Partial passage of products |
Cervix open | Retained uterine products |
| Complete | Vaginal bleeding and complete passage of products |
Cervix open early Cervix closed later |
Empty uterus |
| Missed |
Not many symptoms Brown vaginal discharge |
Cervix closed |
No fetal cardiac activity Non-viable pregnancy |
| Recurrent |
More than 3 miscarriages (Can be any type, incomplete, complete...) |
Variable | Empty uterus and uterine abnormalities may be seen |
- Threatened miscarriage
- Cervical is closed but there is vaginal bleeding before 20 weeks
- Half of these pregnancies will result in a miscarriage but the presence of fetal cardiac activity is a positive sign
- Management
- No effective treatment exists
- Monitoring is done unless the pregnancy is thought to be non-viable
- Inevitable miscarriage
- Vaginal bleeding and an open cervical os before 20 weeks
- Management
- Suction curettage
- Incomplete miscarriage
- Partial expulsion of the fetal products from the uterus before 20 weeks
- Internal cervical os is usually open and allows the passage
- Most common between 6 and 14 weeks
- Management
- Suction curettage
- Complete miscarriage
- Complete expulsion of the fetal products from the uterus before 20 weeks
- Cervical os initially open but closed at the end of complete expulsion
- Most common <6 weeks and >14 weeks
- Management
- Managed expectantly
- Septic abortion
- Fever plus one of threatened, inevitable or incomplete miscarriage before 20 weeks
- Retained products, illegal abortions, and legal abortions can lead to this condition
- Fever can be accompanied by leukocytosis, foul-smelling vaginal discharge, and lower abdominal tenderness
- Can be fatal if sepsis develops
- Management
- Broad-spectrum antibiotics
- Uterine evacuation
- Prostaglandins may be administered to evacuate the uterus to avoid uterine perforation due to infection
- Missed abortion
- Fetal demise before 20 weeks with no detachment from the placenta
- Products are retained for days or even weeks behind a closed cervical os
- Symptoms can be subtle
- Mild bleeding after fetal demise and brown vaginal discharge that follows
- Rarely coagulopathy can ensue in the mother after a prolonged retention
- Management
- Individualized based on the emotional state
- Expectant management can be done but often difficult for the mother
- Medically induced uterine evacuation is commonly the safest option

All information provided on this website is for educational purposes and does not constitute any medical advice. Please speak to you doctor before changing your diet, activity or medications.
